Computational Chemistry-MRI Notes
Magnetic resonance imaging (MRI) is arguably the most sophisticated imaging method
used in clinical medicine. In recent years, MRI scans have become increasingly
common, as costs decrease.
In this article, we will outline the basic principles behind MRI
scans, how to orientate and interpret a scan, and address some of their
advantages and disadvantages compared to other imaging modalities.
Basic Principles
MRI scans work as an imaging method due to the unique make-up of
the human body. We are comprised entirely of cells which all contain water –
principally made of hydrogen ions (H2O).
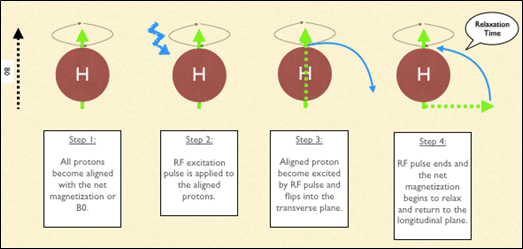
The magnet embedded within the MRI scanner can act on these
positively charged hydrogen ions (H+ ions) and cause them
to ‘spin’ in an identical manner. By varying the strength and
direction of this magnetic field, we can change the direction of ‘spin’ of the
protons, enabling us to build layers of detail.
When the magnet is switched off, the protons will gradually
return to their original state in a process known as precession.
Fundamentally, the different tissue types within the body return at different
rates and it is this that allows us to visualise and differentiate between the
different tissues of the body.
{kind=link}
Fig 1 – MRI scanning is based on the excitation and relaxation of
protons.
Uses of MRI Scanning
Magnetic
resonance imaging can produce highly sophisticated and highly detailed images
of the human body. Generally speaking, MRI scanning is excellent for
visualising soft tissue – and so it is often used in the
detection of tumours, strokes and bleeds. It also can be used to visualise the
functionality of suspected masses and tumours through IV, gadolinium-based
agents.
MRI
scans have many advantages. As stated previously, they provide excellent detail
of the soft tissues of the body, and they do not cause any radiation exposure
to the patient. However, they are time consuming – averaging
approximately 35-45 minutes to complete. This limits their use in trauma and
emergency situations, where CT scanning is often preferred. They are
also by far the most expensive of all the imaging modalities available.
|
Factor |
CT (CT ado used as example) |
MRI |
X-ray (CXR used as example) |
Ultrasound |
|
Duration |
3-7 minutes |
30-45 min |
2-3 min |
5-10 minutes |
|
Cost |
Cheaper |
Expensive |
Cheap |
Cheap |
|
Dimensions |
3 |
3 |
2 |
2 |
|
Soft
tissue |
Poor detail |
Excellent detail |
Poor detail |
Poor detail |
|
Bone |
Excellent detail |
Poor detail |
Excellent detail |
Poor detail |
|
Radiation |
10mSv |
None |
0.15mSv |
None |
At present, there are no known long lasting adverse effects from
MRI scans. However, MRI safety has recently become a major focus in hospital
and outpatient environments due to the potential attraction to ferromagnetic
objects and devices. Some medical and implantable devices are
considered contraindications for MRI evaluation – such as cardiac pacemakers,
heart monitors, defibrillators and other battery-operated devices.
ACTION MECHANISM AND PHARMACOLOGY OF GBCAS
All Gadolinium-Based Contrast Agents (GBCAs) contain the
paramagnetic ion of the rare earth metal gadolinium (Gd3+), which possesses the
most unpaired electrons of any stable ion (seven), creating a high magnetic
moment that is effective at enhancing proton relaxation (Caravan et al., 1999;
Lin et al., 20070.Paramagnetic contrast media shorten the T1 (longitudinal) and
T2(transversal) relaxation times of surrounding water protons to indirectly
produce a signal enhancing effect (Lauffer, 1987). The efficiency of an agent
to shorten relaxation times is called relaxivity, which isdependent on the
ligand surrounding the Gd3+ ion and influenced by extrinsic factors including
temperature,magnetic field strength and the tissue surroundings (water, plasma
or blood). At approved clinical doses ofGBCAs (typically between 0.1 and 0.3
mmol/kg body weight), the T1 relativity effect dominates and yields bright
contrast (Cheng et al., 2012; Lauffer, 19990).Following intravenous injection,
all GBCAs distribute in the blood and extra vascular – extracellular
space (Aime& Caravan, 2009; Staks et al., 1994). GBCAs are biologically
inert and rapidly eliminated by the kidneys, with the exception ofgadoxetic
acid(Primovist®/Eovist®),
gadobenate dimeglumine (Multihance®) and gadofosveset(Vasovist
®/Ablavar ®), which are in part taken up by hepatocytes and
eliminated by the hepatobiliary system.
As Gd3+ ions are toxic, they are chelated with
organic ligands to create GBCAs with either a linear ormacrocyclic structure.
For GBCAs with a linear structure (e.g., Magenvist, Multi Hance, or Ominscan),
a polyamino-carboxylic acid backbone wraps around the Gd
3+ ion, but does not fully enclose it, whereas in macrocyclic chelates
(gadobutrol [Gadovist®], gadoterate meglumine[Ddexzotarem®], and gadoteridol
[Prohance®]), a rigid ―cage‖ with a preorganized cavity surrounds the ion. The
structure of the GBCA determines its complex stability and stability in vivo.
An in vitro study mimicking physiological serum conditions in renally impaired
subjects demonstrated that linear agents,incubated over a 15-day period, could
release substantial amounts of their Gd 3+, while none of the macrocyclic agents
(Gadavist, Dotarem, ProHance) showed detectable Gd 3+ release (<0.1% during
15 days of incubation)
(Frenzel et al., 2008).
This study also demonstrated that for the macrocyclic agents, charge was not
aninfluencing parameter on complex stability. However, in vivo, the
majority of a GBCA dose is excreted within afew days, even in renally
impaired patients; for example, the elimination half-life of gadobutrol is 90
min inhealthy subjects (Staks et al., 994) and 7 – 26 h in those with
kidney disease (Frenzel et al., 2008; Tombach et al.,2000).
DEVELOPMENT AND CHARACTERISTICS OF MR
CONTRAST AGENTS
After the introduction of gadopentetate dimeglumine, the use of CE-MRI as a diagnostic
imaging tool has expanded rapidly. While it was understood that Gd 3+ was the
most effective paramagnetic ion for proton relaxation, other paramagnetic ions
have been developed for use as MRI contrast agents, including Mn 2+ (Bernardion
et al., 1992) and iron oxide compounds (Stark et al., 1988). Today, contrast
media are administer edin about 25% of all MRI examinations, especially for the
brain and spine, for MR angiography (MRA) and forMRI of the abdomen, breast and
heart (Ferre et al., 2012).Five further extracellular GBCAs, exhibiting the
same, passive distribution and renal excretion as gadopentetate dimeglumine,
have been approved for clinical use (Restrepo et al., 2012; Serrano et al.,
2012)gadoterate (1989), gadoteridol (1992), gadodiamide (Omniscan ®; 1993),
gadobutrol (1998) and gadoversetamide (Optimark™; 1999). With the approval of
gadobenate (1998) and gadoxetic acid (2005), two agents entered the market which
exhibited a different pharmacokinetic profile to the other GBCAs— in
addition to extracellular distribution, these agents are taken up to different
degrees by hepatocytes, and thus produce a unique enhancement of liver
parenchyma with partial excretion in the bile. A third group of agents are
those which, after intravenous injection, remain in the circulation for
prolonged periods, allowing extend edimaging times for MRA. These
agents include gadofosveset and the ultra small superparamagnetic
iron oxide (USPIO) particles (which have
limited commercial availability) (Bremerich et al.,2007)Gadolinium-based
contrast agents differ in their ability to shorten relaxation times, as a
function oftheir relaxivity and local tissue concentration (Rohrer et al., 2005)
Gadobutrol was considered a ‗second -generation‘ GBCA (Scott, 2013) owing to
its higher concentration and relatively high relaxivity (and thus
improved imaging capacity) compared with earlier agents.
(Gadobutrol is the only GBCA formulated at a concentration of 1.0 M, twice that
of other agents. Combined with its high relaxivity in plasma,
gadobutrol provides the greatest T1 shortening per volume of
any currently available GBCA (Sieber, 2009).
Comments
Post a Comment